The success of CAR-Ts in oncology has stoked enthusiasm for developing comparable curative therapies in other disease areas. CellProthera’s Chief Scientific Officer, Ibon Garitaonandia, explains the potential and progress for CGTs in cardiology, where disease-modifying therapies are largely non-existent.

Cell and gene therapies (CGTs) have made significant advancements in treating oncological diseases, with therapies like CAR-T cell treatments transforming cancer care. However, innovation and scientific progress are rapidly broadening the scope of CGT applications, extending into non-oncological areas such as cardiology, where there is enormous potential for addressing unmet clinical needs.
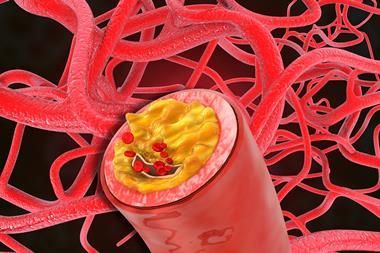
Cardiovascular diseases are the leading cause of mortality worldwide, and traditional approaches like drug therapy or invasive procedures manage symptoms but do not restore lost cardiac tissue. In acute myocardial infarction (AMI), for example, a blocked artery leads to necrosis of muscle cells and loss of contractility, which leads to remodeling and, eventually, heart weakening. Severe heart attacks, which occur in 30 percent of all AMI patients, can lead to chronic heart failure with high mortality despite medication. In severe AMI patients with multiple risk factors such as microvascular obstruction, left ventricular dysfunction, and high cardiac biomarkers, mortality and heart failure readmission remain high, around 15 percent per year. There are approximately 50 million people worldwide living with chronic heart failure and approximately 50 percent of AMI patients die within five years of a heart attack.
Symptom management through the standard of care includes lifelong treatments with drugs such as renin-angiotensin, beta blockers, aldosterone system inhibitors, and SGLT2 inhibitors. Medical devices, such as a left ventricular assist device, carry the risk of mechanical failure and formation of blood clots within the devices. Heart transplantation is an option if all others fail, but it is limited by a lack of donors and the risks associated with surgery. This leaves room for innovative solutions like CGTs, but their development faces unique challenges that must be addressed for widespread adoption and success.
Cell and gene therapies for cardiovascular diseases
The expansion of CGTs into cardiology stems from advances in cellular reprogramming, gene editing, and delivery technologies. Unlike conventional therapies, CGTs offer the potential for regenerative treatment, aimed at not only managing symptoms but also repairing damaged heart tissue and correcting underlying genetic defects.
The heart does have limited regenerative capacity, but not enough of the healthy cells that capable of restoring function, making it difficult to recover from injuries such as myocardial infarction. However, cell-based therapies are intended to leverage those healthy cells via transplant to regenerate damaged tissue.
Tissue engineering techniques using induced pluripotent stem cells (iPSC), which are differentiated into cardiomyocytes, are being developed to create functional cardiac tissues from patient-derived cells. Innovations in biomaterials for scaffolds and hydrogels support cell survival and integration when transplanted into the heart tissue.
Stem cell-based therapies using CD34+ stem cells and mesenchymal stem cells promote cardiac tissue repair by secreting growth factors and anti-inflammatory signals that aid tissue recovery. After an AMI, the damaged heart tissue secretes chemokines that mobilise CD34+ cells from the bone marrow to peripheral blood. The concentration of CD34+ cells in the peripheral blood after AMI is significantly correlated with heart regeneration and functional improvement. Once mobilised, CD34+ cells home to the ischemic lesion and release paracrine factors that induce angiogenesis and revascularisation of the damaged tissue. They also engraft in the ischemic zone and begin their commitment into the endothelial pathway, further promoting revascularisation.
By harvesting, expanding, and injecting CD34+ cells directly to the heart muscle, this natural repair mechanism is enhanced. Early-phase clinical trials have shown the safety and efficacy of using stem cells for cardiac repair, encouraging further research and development.1
Gene therapies for cardiology aim to address genetic causes of cardiovascular diseases or modify cellular behaviour in the heart to promote regeneration or prevent damage. These therapies can modulate pathways involved in cardiac regeneration, protect against ischemic injury, or promote angiogenesis. This approach can be highly targeted, with the potential to correct mutations that lead to specific diseases or deliver therapeutic genes to improve heart function.
Advances in genomics have enabled the identification of patient-specific genetic mutations, allowing for tailored gene therapies. CRISPR-Cas9 and other gene-editing technologies enable precise editing of genetic defects responsible for inherited heart diseases, such as hypertrophic cardiomyopathy or dilated cardiomyopathy. By correcting these mutations, gene-modifying and editing therapies hold the promise of long-term, potentially curative treatments.
Viral vectors, such as adeno-associated viruses (AAVs), are commonly used to deliver therapeutic genes to cardiac cells. RNA-based therapies, including mRNA and RNA interference (RNAi), are being explored to modulate gene expression in heart cells. For instance, mRNA therapies can promote the production of specific proteins required for heart tissue repair, while RNAi can silence harmful gene expression, such as those driving fibrosis in heart failure.
Challenges for CGT development in cardiology
While CGTs hold great promise for cardiology, the field faces numerous scientific and technical challenges that must be overcome to translate potential into widespread clinical success.
Cardiovascular diseases often involve multiple cell types and large areas of tissue damage, as seen with heart failure or ischemic heart disease. Achieving sufficient cellular integration, proliferation, and functionality within the complex architecture of heart tissue remains a significant hurdle. When transplanting cardiomyocytes or their stem cell progenitors, the cells must not only survive but also integrate functionally with existing tissue to restore contractility and rhythm. If the transplanted cardiomyocytes beat at a different rhythm, arrhythmias may occur.
One of the most critical challenges for CGTs in cardiology is the efficient and targeted delivery of therapeutic agents. Unlike oncology, where localised tumours are more accessible, cardiovascular diseases affect large, moving organs. Delivering stem cells to the heart in sufficient numbers and ensuring their retention in the hostile environment of damaged heart tissue is challenging, leading to low survival rates for transplanted cells. Intravenous administration often leads to cells being trapped in other organs, such as the lungs or liver, rather than reaching the heart.
Several approaches are designed to circumvent these obstacles. For cell-based therapies, direct intramyocardial injections using minimally invasive techniques such as transendocardial catheter-based delivery allow direct delivery to the heart, increasing efficiency and cell retention rates.2 Improved imaging technologies also help track transplanted cells and assess therapy efficacy.
For gene therapies, the main challenge lies in ensuring that viral or non-viral vectors reach heart cells efficiently without being neutralised by the immune system. While commonly used, AAVs have limitations, including immune reactions and difficulties with re-dosing due to pre-existing antibodies. Nanoparticles for gene delivery can improve targeting and reduce immunogenicity.
As with all CGTs, safety concerns, particularly related to immune responses and long-term effects, are crucial in cardiology. Allogeneic cell therapies must avoid immune rejection. Preconditioning these cells before transplantation to enhance their survival and integration or encapsulating them in biocompatible materials may shield them from the inflammatory environment. Gene therapies must be designed to minimise off-target effects and ensure the stability of the introduced genetic material. For example, integrating gene therapies that alter the DNA of cardiac cells pose risks of unintended genetic modifications, which could lead to tumorigenesis.
Real-world challenges for cardiac CGT
Regulatory frameworks for CGTs, especially in cardiology, are still evolving. The complex nature of biologics, combined with innovative gene-editing techniques, raises concerns about long-term safety and efficacy, requiring more stringent and prolonged clinical trials. Scaling manufacturing up or out from early-stage research to large-scale production of CGTs, particularly cell-based therapies, poses substantial challenges. Ensuring consistency, purity, and scalability of cell therapies is critical, particularly for autologous therapies, where cells are sourced from individual patients and must be processed to meet therapeutic standards.
Therefore, it is critical to develop robust analytical methods to ensure product quality and safety. Fortunately, regulatory agencies can provide guidance and have introduced pathways to expedite the development and approval of CGTs for serious conditions with unmet medical needs.
Still, the high cost of CGTs, driven by their complexity and individualised nature, presents barriers to widespread adoption in cardiology, limiting patient access. Autologous cell therapies, which involve extracting, manipulating, and reinfusing a patient’s own cells, are resource-intensive and expensive. Innovation in automation, supply chain management, and process standardisation will be essential to reduce costs and improve accessibility. Collaborative efforts between public and private entities might provide the resources and expertise needed to advance CGT development.
Future directions
Despite these challenges, the future of CGTs in cardiology is promising. Continued growth in the field relies on multidisciplinary efforts combining biology, engineering, and clinical medicine. Ongoing innovation in stem cell biology, gene editing, delivery technologies, and advanced biomaterials is likely to address many of the current obstacles.
Moreover, advancements in automation and biomanufacturing may help scale these therapies while improving consistency and reducing costs. Combining cell therapy with biomaterials, such as cardiac patches or scaffolds, may enhance cell retention and integration. These engineered tissues can be implanted to promote heart regeneration while providing structural support.
The development of off-the-shelf allogeneic therapies, where cells are sourced from healthy donors, could make CGTs more accessible and scalable. Techniques such as gene editing are being explored to reduce the immunogenicity of allogeneic cells, allowing for broader use without rejection.
CGTs have the potential to revolutionise the treatment of cardiovascular diseases by offering regenerative solutions that go beyond symptom management. While the field faces significant challenges related to efficacy, delivery, safety and cost, ongoing scientific innovations and advancements in manufacturing are steadily overcoming these barriers. By addressing these challenges, CGTs could become a transformative approach to cardiac care, offering hope for millions of patients with otherwise untreatable heart conditions.
References
1 CellProthera | CellProthera announces positive Phase I/IIb data for ProtheraCytes® cell therapy in acute myocardial infarction [Internet]. Cellprothera.com. 2024 [cited 2024 Sep 11]. Available from: https://www.cellprothera.com/en/cellprothera-announces-positive-phase-i-iib-data-for-protheracytes-cell-therapy-in-acute-myocardial-infarction/
2 Mitsutake Y, Pyun WB, Rouy D, Foo CWP, Stertzer SH, Altman P, Ikeno F. Improvement of Local Cell Delivery Using Helix Transendocardial Delivery Catheter in a Porcine Heart. Int Heart J. 2017 May 31;58(3):435-440. doi: 10.1536/ihj.16-179. Epub 2017 May 23. PMID: 28539564.
About the author
 Ibon Garitaonandia, PhD is Chief Scientific Officer at CellProthera, a French clinical-stage biotechnology company developing stem cell-based therapies for ischemic diseases. Ibon is a seasoned executive with several years of experience in the cell therapy field. Prior to CellProthera, he developed therapies for Parkinson’s disease, traumatic brain injury and other indications. CellProthera recently completed a successful Phase II study in AMI and is preparing to launch a pivotal Phase III study.
Ibon Garitaonandia, PhD is Chief Scientific Officer at CellProthera, a French clinical-stage biotechnology company developing stem cell-based therapies for ischemic diseases. Ibon is a seasoned executive with several years of experience in the cell therapy field. Prior to CellProthera, he developed therapies for Parkinson’s disease, traumatic brain injury and other indications. CellProthera recently completed a successful Phase II study in AMI and is preparing to launch a pivotal Phase III study.