



Tau tangles are a hallmark of Alzheimer’s disease and related disorders, but evidence suggests the real damage may come from rare, soluble tau species inside neurons. Targeting these hidden drivers of circuit dysfunction could be key to restoring memory and cognition.

Tau is one of the most challenging therapeutic targets in neurodegeneration. Central to the biology of primary tauopathies, it contributes to disorders in which other proteins accumulate alongside it, notably Alzheimer’s disease (AD).
In recent years, much of the field’s focus has centred on detecting and tracking tau pathology, including where it is present and how it is distributed across the brain. However, far less work has been dedicated to defining which tau species contribute to neural system dysfunction and which represent prime targets for removal. This is now a central challenge for drug discovery.
Tau is a normal intracellular protein, mainly associated with axonal microtubules. In disease, it leaves its usual compartment, loses normal function and promotes harmful interactions elsewhere in the neuron. It also becomes abnormally modified, appears outside cells and exists in multiple forms that differ in solubility, size, localisation and bioactivity. Some forms are filamentous and visible as inclusions. Others remain soluble and are much harder to define structurally. For drug discovery, a key question is which tau species to target, in which compartment and how to do so without disrupting normal tau function.
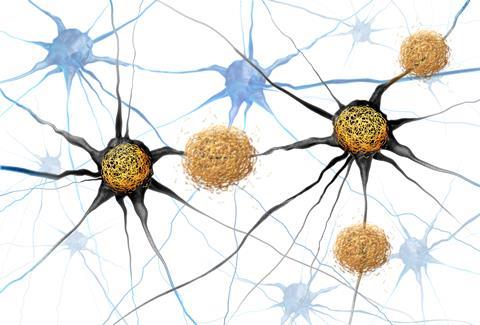
Tau is a protein found in neurons that normally supports axonal structure and transport. In tauopathies and Alzheimer’s disease, tau becomes abnormally modified and accumulates in forms that disrupt neuronal and circuit function. Credit: Shutterstock / Lightspring
For many years, visible tau inclusions have provided a dominant framework for thinking about toxicity. Neurofibrillary tangles and related fibrillar lesions are defining hallmarks across tauopathies, and they are easy to see, stage and quantify. But visibility need not necessarily imply biological relevance. Increasingly, the field is being pushed towards a less convenient but more important question: is the most obvious tau pathology also the most actionable one? That concern is strengthened by neuropathological observations showing that neuronal loss can substantially exceed the number of tangles, suggesting that fibrillar tau may correlate with degeneration without necessarily being its main or direct mediator.1 This raises the possibility that much of the most relevant tau biology may reside in forms of tau that are biochemically detectable but not visible by classical fibrillar labelling.
One reason the answer to the above question may be “no” comes from functional studies. Our earlier in vivo work showed that tau can profoundly suppress cortical neuronal activity and silence large numbers of neurons, and that this dysfunction can be reversed by suppressing soluble tau even when tangles remain present.2 This fits with a broader literature suggesting that tangle burden does not map in a simple way onto neuronal dysfunction at the single-cell level and that neurons carrying tangles can remain functionally integrated for surprisingly long periods.3-5 Together, these observations argue against a simple tangle-centric model of toxicity. They also raise a practical concern for drug discovery. A therapy that merely disrupts fibrillar aggregates, without reducing the relevant soluble species, could potentially increase the pathogenic soluble tau pool.
That proposition raises another question: if tangles are not enough to buttress a drug discovery framework, which soluble tau species should be prioritised instead?
The case for soluble tau species
One candidate attracting attention is a rare, soluble, high molecular weight (HMW) form of hyperphosphorylated tau. This species matters because very small amounts appear sufficient to impair neuronal and circuit function. It was first defined in human AD brain, where it can be isolated from the soluble fraction and separated from the far more abundant low molecular weight (LMW) monomeric and dimeric tau pool.6,7 Similar HMW soluble tau species have now been reported in primary tauopathies, such as progressive supranuclear palsy (PSP), suggesting that this is not unique to AD.8
Soluble tau is a heterogeneous population in which a very small fraction may carry disproportionate biological activity. HMW tau is especially important because it is bioactive and can move between neurons, seed further tau aggregation and has been linked to the rate of clinical progression in people with AD.9 By contrast, LMW tau appears far less potent in these respects. For therapeutic development, that distinction may matter more than simply the total amount of tau present.
We developed an experimental platform that allowed us to introduce patient-derived HMW tau into individual hippocampal neurons while recording their activity.
In our recent work, we investigated whether this rare soluble species can impair neuronal function relevant to cognition. This is important since the action potential, or spike, is the basic unit of neuronal communication and changes in spike output provide a direct readout of how a molecular abnormality can influence downstream circuits. To address this, we developed an experimental platform that allowed us to introduce patient-derived HMW tau into individual hippocampal neurons while recording their activity.10 The result was striking. Low nanomolar concentrations of HMW tau were sufficient to suppress complex spike bursts – rapid sequences of action potentials that are important for synaptic plasticity, learning and memory. Recent work suggests that these bursts depend on dendritic events that help drive rapid synaptic plasticity in CA1,11 raising the possibility that HMW tau disrupts not only firing, but also a mechanism needed for memory formation. Notably, this was not a non-specific depression of neuronal activity. Single spiking was relatively preserved, while bursting was selectively impaired. Tau is not simply lowering activity overall; it is selectively disrupting a firing pattern that is important for learning and memory.
Tau, bursting and memory circuits
Mechanistically, impaired bursting was associated with reduced expression of CaV2.3 R-type calcium channels, which are important for burst generation in hippocampal neurons.10 These changes were accompanied by disruption of hippocampal network activity, including reduced ripple events and altered theta-related coupling, both of which are closely linked to memory processing. Importantly, the phenotype was not reproduced by LMW tau from the same AD brain extract, nor by tau immunodepleted fractions. It was also not dependent on mature tangles. Lowering soluble tau in vivo restored both CaV2.3-related changes and burst firing deficits, without requiring removal of tangles. Together, these findings suggest that rare soluble tau species, present at low abundance intracellularly, can have a specific, reversible and biologically meaningful effect on neuronal physiology.
We have also recently shown that tau-related impairment of burst output is not confined to the hippocampus.12 In the neocortex, bursting is selectively reduced in superficial layers and this physiological deficit maps onto the cortical layers in which tau pathology is most prominent. The downstream deficit appears to involve reduced synaptic localisation of NMDA receptors, including loss of the obligatory GluN1 subunit and a similar reduction in synaptic GluN1 is detectable in human AD tissue. Together, these data suggest that tau can degrade memory-related circuit function through more than one downstream mechanism, including synaptic NMDAR loss.
We have also recently shown that tau-related impairment of burst output is not confined to the hippocampus.
Our data also argue strongly that intracellular localisation matters. In our experiments, the toxic effect emerged when patient-derived HMW tau entered the neuron, while LMW tau and immunodepleted fractions did not reproduce the phenotype. This suggests that a successful tau therapy may need to reduce or neutralise intracellular pathogenic tau, not merely extracellular tau or bulk tau burden. Thus, strategies that reduce the generation, persistence or intracellular activity of pathogenic soluble tau, while sparing normal tau function as much as possible, are likely high priority. Extracellular tau may still matter for propagation between cells and it may still be a useful therapeutic entry point. But if the key dysfunction occurs inside neurons, then therapies that do not meaningfully affect that intracellular pathogenic pool may have limited impact on neuronal function. An important toxic tau pool may sit near synapses and current fibril-based readouts may miss it.13,14
Implications for drug development
This has direct implications for drug development. Tau programmes have largely prioritised pathology burden and biochemical engagement, such as total tau, phospho-tau, seed amplification and aggregate load. These measures are useful but may not be sufficient on their own. A tau-directed therapy may change tau biochemistry without restoring the physiological functions that matter most for cognition. For that reason, assays should define tau species more precisely, rather than treating tau as a single undifferentiated analyte, resolving soluble species by properties such as size, localisation and bioactivity wherever possible. In our work, separation of HMW from LMW soluble tau provides one example of why this matters. Assays should also include functional readouts such as spiking, burst firing, network oscillations, or linked channel and receptor phenotypes. In our research, CaV2.3-related burst impairment provides one example of such a readout. In other settings, other physiological signatures may prove more informative. Success should not be defined solely by target engagement, but by recovery of neuronal and circuit function that underpins cognitive processes.
Assays should define tau species more precisely, rather than treating tau as a single undifferentiated analyte.
One of the persistent problems in neurodegeneration research is the gap between model systems and human disease. Behavioural readouts in animals are useful, but they are often distant from the underlying biology and difficult to align directly with clinical trials. At the same time, fluid biomarkers and molecular imaging are valuable for showing whether pathology is present, but they are relatively distal from cognition itself. Symptoms emerge when pathology disrupts the circuits that support memory and thought. Circuit physiology may therefore sit closer to cognition than fluid biomarkers or molecular imaging. In sum, pathology markers tell us that disease biology is present, but circuit-level markers may tell us when that biology is beginning to matter for cognition. Importantly, advanced computational analyses are beginning to increase the information that can be extracted from EEG and MEG scanning.15,16 Rather than only measuring broad features such as slowing or oscillatory power, these approaches can detect more specific and temporally structured signatures of circuit function from non-invasive recordings. That creates the possibility that tau-directed therapies could be evaluated not only through fluid biomarkers and imaging, but also through restoration of neural system function. This may be especially valuable in early-stage disease, when cognition remains relatively preserved but circuit dysfunction is already emerging.
Different challenges across tauopathies
The therapeutic context differs across diseases. In primary tauopathies, where tau is the central aggregating protein, precise targeting of pathogenic soluble tau may be especially attractive. In disorders with mixed proteinopathy, such as AD, the picture is more complicated. Our earlier in vivo work suggested that tau lowering alone may be substantially less effective when amyloid beta is present at the same time, implying that once dual proteinopathy is established, combination approaches may be needed.2,12 The core lesson remains the same: tau should not be treated as a single undifferentiated target. The pathogenic species, the disease stage and the intracellular versus extracellular compartment are all likely significant.
The field should therefore judge the next generation of tau therapeutics less by their effect on tangles alone and more by whether they reduce intracellular pathogenic soluble tau species and restore defined neuronal functions. Tau drug discovery now requires two changes in emphasis. The first is a move away from visible fibrillar pathology towards the rare intracellular soluble tau species that appear to be most functionally toxic. The second is a move away from biochemical target engagement as an endpoint and towards demonstrable recovery of neuronal and circuit function. Neuropathology and biochemistry have taken the field a long way, but they are not sufficient on their own.
The central questions are now functional: Which tau species are truly bioactive? Where do they act? What physiological signatures do they disrupt? And can those signatures be restored in a way that translates from experimental models to patients? If the field can answer those questions, soluble intracellular tau may become not just a pathological concept but a tractable and clinically meaningful therapeutic target across the tauopathies.
References
1. Gomez-Isla T, et al. Neuronal loss correlates with but exceeds neurofibrillary tangles in Alzheimer’s disease. Ann Neurol 41, 17-24 (1997). https://doi.org/10.1002/ana.410410106
2. Busche MA, et al. Tau impairs neural circuits, dominating amyloid-beta effects, in Alzheimer models in vivo. Nat Neurosci 22, 57-64 (2019). https://doi.org/10.1038/s41593-018-0289-8
3. Marinkovic P, et al. In vivo imaging reveals reduced activity of neuronal circuits in a mouse tauopathy model. Brain 142, 1051-1062 (2019). https://doi.org/10.1093/brain/awz035
4. Kuchibhotla KV, et al. Neurofibrillary tangle-bearing neurons are functionally integrated in cortical circuits in vivo. Proc Natl Acad Sci U S A 111, 510-514 (2014). https://doi.org/10.1073/pnas.1318807111
5. Zwang TJ, et al. Neurofibrillary tangle-bearing neurons have reduced risk of cell death in mice with Alzheimer’s pathology. Cell Rep 43, 114574 (2024). https://doi.org/10.1016/j.celrep.2024.114574
6. Takeda S, et al. Neuronal uptake and propagation of a rare phosphorylated high-molecular-weight tau derived from Alzheimer’s disease brain. Nat Commun 6, 8490 (2015). https://doi.org/10.1038/ncomms9490
7. Hyman B. All the Tau We Cannot See. Annu Rev Med 74, 503-514 (2023). https://doi.org/10.1146/annurev-med-042921-023749
8. Martinez-Valbuena I, et al. 4R-tau seeding activity reveals molecular subtypes in progressive supranuclear palsy. Nat Commun 17, 1006 (2025). https://doi.org/10.1038/s41467-025-67744-y
9. Dujardin S, et al. Tau molecular diversity contributes to clinical heterogeneity in Alzheimer’s disease. Nat Med 26, 1256-1263 (2020). https://doi.org/10.1038/s41591-020-0938-9
10. Harris SS, et al. Alzheimer’s disease patient-derived high-molecular-weight tau impairs bursting in hippocampal neurons. Cell 188, 3775-3788 e3721 (2025). https://doi.org/10.1016/j.cell.2025.04.006
11. Bittner KC, Milstein AD, Grienberger C, et al. Behavioral time scale synaptic plasticity underlies CA1 place fields. Science 357, 1033-1036 (2017). https://doi.org/10.1126/science.aan3846
12. Ellingford R, et al. Alzheimer’s disease pathology degrades an NMDA receptor-dependent spontaneous activity pattern in cortico-hippocampal circuits. Neuron (2026). https://doi.org/10.1016/j.neuron.2026.02.027
13. Fertan E, et al. Early synaptic pathology is associated with small tau aggregates in Alzheimer’s disease. Acta Neuropathol 151, 7 (2026). https://doi.org/10.1007/s00401-026-02977-9
14. McGeachan RI, et al. Evidence for trans-synaptic propagation of oligomeric tau in human progressive supranuclear palsy. Nat Neurosci 28, 1622-1634 (2025). https://doi.org/10.1038/s41593-025-01992-5
15. Liu Y, Dolan RJ, Kurth-Nelson Z, Behrens TEJ. Human Replay Spontaneously Reorganizes Experience. Cell 178, 640-652 e614 (2019). https://doi.org/10.1016/j.cell.2019.06.012
16. Chen Z, et al. Interpreting human sleep activity through neural contrastive learning. Neuron (2026). https://doi.org/10.1016/j.neuron.2026.03.028














No comments yet