



Despite decades of research, advanced ovarian cancer remains defined by recurrence and poor survival. Synthetic induced pluripotent stem cell-derived mesenchymal stem cells (iMSCs) are emerging as a promising new approach to reprogramme the tumour microenvironment and restore anti-tumour immunity.
Ovarian cancer was responsible for nearly 13,000 deaths in 2025 in the US,1 making it the fifth leading cause of cancer death for women.2 Despite decades of research, the standard of care − aggressive surgery to debulk the tumour followed by platinum-based chemotherapy − has changed little and outcomes have not meaningfully improved for women with advanced disease.3
Though most patients respond to first-line therapy, resistance and relapse are common, partly because most patients are diagnosed at an advanced stage (stage III or IV) when the disease has already spread. For women with advanced ovarian cancer, the disease will return for 70–80 percent – often more aggressively than before.3 The five-year survival rate for stage IV is just 31.5 percent.4
A key driver of recurrence is the presence of cancer stem cells (CSCs), a rare subpopulation of tumour cells that resist chemotherapy and whose capacity for self-renewal, adaptability and tumour regeneration allows them to evade treatment and regenerate tumours.5
The role of the tumour microenvironment
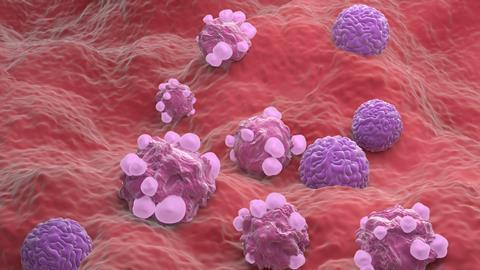
A crucial role in maintaining ovarian cancer stem cells (OCSCs) is played by the tumour microenvironment (TME) – an intricate fibre network made up of cancer cells, immune cells and the extracellular matrix. The TME provides structural support, integrates local signals and regulates cellular movement, proliferation and differentiation.5-7
The TME functions as an accomplice to the progression of disease by harbouring immune-suppressive cells and inflammatory mediators, even after therapy.5 It creates a pro-tumourigenic niche encased in a dense extracellular matrix and fibrotic stroma (dense, stiff fibrotic tissue), which acts as a fortress-like barrier against drug delivery. This promotes OCSC maintenance, invasion and chemoresistance, thereby increasing OCSC survival and progression.
While conventional therapies have shown efficacy against bulk tumour cells, they can inadvertently promote the expansion of OCSCs.5 As one researcher put it, cancer cells “conscript resident and normal cell types to serve as contributing members to the outlaw society of cells.”6
The pro-tumourigenic nature of the TME in ovarian cancer helps explain why so many promising treatments have failed to deliver. Immune checkpoint inhibitors, for instance – a type of immunotherapy that blocks checkpoint proteins which cancer cells exploit to evade the immune system – have revolutionised the treatment of melanoma and lung cancer, but have demonstrated only modest benefit in ovarian cancer.
The pro-tumourigenic nature of the TME in ovarian cancer helps explain why so many promising treatments have failed to deliver.
The situation is similar for angiogenesis inhibitors, which block the formation of new blood vessels that tumours need to grow and spread, and PARP inhibitors, which promote cancer cell death by preventing cancer cells from repairing DNA damage. Both therapies offer incremental gains for select ovarian cancer patient subgroups, but not a paradigm shift. For most women, available therapies extend survival by months, not years.
Given the limitations of current treatments for advanced disease, researchers are turning to OCSCs to examine their pivotal role in drug resistance and tumour relapse.5
Remodelling the tumour microenvironment
Mesenchymal stem cells (MSCs) are a type of adult stem cell found in various tissues throughout the body. They have long attracted the interest of researchers for their natural ability to migrate towards tumours and inflammation sites, suggesting a potential therapeutic strategy: engineering MSCs to carry anti-cancer payloads directly into tumours, thereby bypassing systemic barriers.
The ovarian cancer TME is dominated by factors that allow the tumour to evade immune destruction by suppressing effector T cells and natural killer (NK) cells. These factors include regulatory T cells, myeloid-derived suppressor cells and inhibitory cytokines such as transforming growth factor-beta (TGF-β) and interleukin-10 (IL-10).
Synthetic induced pluripotent stem cell-derived mesenchymal stem cells (iMSCs) engineered to secrete beneficial cytokines such as IL-7 and IL-15 could create a more balanced TME environment. IL-7 supports T-cell survival and proliferation, while IL-15 enhances NK and memory T-cell activation. Together, they could invigorate exhausted immune cells within the TME, restore cytotoxic activity and drive deeper tumour infiltration.
The use of synthetic iMSCs to reprogramme the TME addresses the two major challenges in treating ovarian cancer: immune evasion and poor penetrability. Rather than serving as a sanctuary for tumour growth, the TME could become a hub for anti-tumour immunity.
The evolution of synthetic iMSCs
Early studies demonstrating that MSCs could deliver cytokines, prodrugs (which convert to a parent drug in the body), or other agents to tumours were encouraging. However, limitations emerged when they advanced towards the clinic. Traditional MSCs, which are harvested from bone marrow or adipose tissue, exhibited variable potency depending on the donor or donors. They also often failed to persist long enough in vivo to be effective and, being non-autologous, could trigger immune rejection.8
While autologous approaches, which use the patient’s own MSCs, were more effective, they were also impractical. The time, cost and complexity associated with harvesting, expanding and engineering cells for each individual patient made the therapy difficult to scale for widespread use. For these reasons, the promise of MSC-based therapeutics was never realised, despite their elegant scientific rationale.
Recent advances in stem cell biology, however, have opened the door to a new generation of MSC-based therapeutics. The groundbreaking discovery of induced pluripotent stem cells (iPSCs) by Shinya Yamanaka and colleagues in 2006, which earned Yamanaka the Nobel Prize, demonstrated that mature human somatic cells could be reprogrammed to a pluripotent, embryonic stem cell-like state, allowing them to be transformed into nearly any cell type.
By guiding iPSCs into mesenchymal stem cell fate, scientists could create “induced” – or synthetic – MSCs (iMSCs). These synthetic iMSCs are distinctive not only because of their origin, but also because they can be bioengineered at genetic and functional levels. In ovarian cancer, for instance, they can be optimised to overcome the limits of earlier MSC approaches. The advantages of iMSCs include: 8,9
- Consistency, scalability and low heterogeneity: synthetic iMSCs can be generated from homogeneous, well-characterised clonal cell lines under tightly controlled conditions and expanded indefinitely, creating uniform, bankable batches for multiple patients. Their high proliferative capacity and delayed senescence further support large-scale manufacturing while minimising the variability commonly seen with MSCs derived from multiple donors.
- Streamlined and stable genetic engineering: genetic modifications can be introduced at the iPSC stage, where cells are highly amenable to engineering, before differentiation into iMSCs. This approach enables the creation of more consistent and precisely engineered therapeutic cell products.
- Immune compatibility and durable persistence: because their immunological profile can be engineered and controlled, synthetic iMSCs may resist rapid immune clearance and persist in vivo long enough to deliver meaningful therapeutic effects. Immune-evasive engineering strategies may further enhance durability and therapeutic activity within the body.
- Enhanced tumour homing: iMSCs retain the natural migratory cues of MSCs, which are guided by chemokine gradients released from tumours, enabling targeted trafficking to sites of disease.
- Localised payload delivery: perhaps most importantly, iMSCs can be engineered to secrete potent immune-activating cytokines, including IL-7 and IL-15, directly within the TME, helping concentrate therapeutic activity at the tumour site while potentially reducing systemic toxicity.
By guiding iPSCs into mesenchymal stem cell fate, scientists could create “induced” – or synthetic – MSCs.
The ability to deliver cytokines directly to the tumour site solves the problem of systemic toxicity that has long plagued cytokine therapy. While IL-7 and IL-15 have demonstrated strong anti-tumour activity in principle, when delivered intravenously, their use has been limited by dangerous side effects, preventing their clinical adoption to date. But synthetic iMSCs are designed to capture the therapeutic benefits of these molecules while minimising their risks.10
At the 2025 American Society of Clinical Oncology (ASCO) Annual Meeting, preclinical data was presented, showing that synthetic iMSCs could indeed infiltrate ovarian tumours and deliver immune-activating cytokines in situ. In mouse models, tumours treated with engineered iMSCs exhibited increased T-cell proliferation and infiltration, reduced markers of T-cell exhaustion and tumour regression compared with controls.10
Importantly, these benefits were achieved without systemic cytokine-related toxicities, underscoring the value of localised delivery. While these findings remain preclinical, they provide a strong rationale for advancing synthetic iMSCs into clinical trials.11
Looking ahead
Synthetic iMSCs are showing great promise. Synergistic combination regimens may target not only cancer cell-intrinsic pathways, but also cancer cell-extrinsic cells, pathways and mediators in the TME.5,6 By circumventing adaptive mechanisms, such integrative approaches could profoundly alter the prognosis for advanced ovarian cancer patients by more thoroughly extinguishing primary and metastatic disease, turning incremental benefits into long-lasting responses.6
Combination regimens include:
- With adoptive cell therapies: iMSCs may help enhance the activity and persistence of adoptive immune cell therapies, including CAR-NK cells, CAR-T cells and tumour-infiltrating lymphocytes (TILs), by reshaping the TME to better support sustained immune activity
- With T-cell engagers: combining iMSCs with T-cell engagers, such as bispecific T-cell engagers (BiTEs), may help improve immune-cell recruitment and activation within the tumour, potentially strengthening anti-tumour responses
- With therapeutic vaccines: therapeutic cancer vaccines are designed to prime tumour-specific immune responses, while iMSCs may help amplify and sustain those responses within the TME through localised cytokine delivery and immune modulation
- With checkpoint inhibitors: by reinvigorating T cells within the TME, iMSCs may amplify the benefits of checkpoint blockade and help overcome immune suppression within solid tumours.
While the benefits of synthetic iMSCs for ovarian cancer provide compelling proof of concept, their implications extend further. Many solid tumours, including pancreatic, colorectal and glioblastoma, share similar challenges: dense stroma, immunosuppressive TMEs and poor responses to checkpoint inhibitors. Synthetic iMSCs may also serve as a platform technology to address these cancers.
The opportunity posed by synthetic iMSCs is profound. After decades of incremental progress in ovarian cancer, they offer a fundamentally different approach: by infiltrating the TME and turning it against the disease, iMSCs can overcome chemoresistance, reduce the rate of recurrence and improve survival outcomes for patients with advanced-stage ovarian cancer.5
Rather than fighting the tumour from the outside, iMSC therapy is a potential Trojan horse that allows the body to fight the tumour from the inside out with tools to reprogramme the TME and reawaken the immune system. For patients with advanced disease who face a 70 percent chance of recurrence after frontline therapy, this innovation may one day offer a potential second chance.
References:
1. American Cancer Society: Key Statistics for Ovarian Cancer, https://www.cancer.org/cancer/types/ovarian-cancer/key-statistics.html
2. Siegel RL, Kratzer TB, Giaquinto AN, et al. Cancer statistics, 2025. CA Cancer J Clin. 2025; 75(1): 10-45. doi:10.3322/caac.21871
3. Matulonis UA, Sood AK, Fallowfield L, et al. Ovarian cancer. Nat Rev Dis Primers. 2016 Aug 25;2:16061. doi: 10.1038/nrdp.2016.61. PMID: 27558151; PMCID: PMC7290868
4. Alizadeh H, Akbarabadi P, Dadfar A, et al. A comprehensive overview of ovarian cancer stem cells: correlation with high recurrence rate, underlying mechanisms, and therapeutic opportunities. Mol Cancer 24, 135 (2025). https://doi.org/10.1186/s12943-025-02345-3
5. Hanahan D, Coussens LM. Accessories to the crime: functions of cells recruited to the tumor microenvironment. Cancer Cell. 2012 Mar 20;21(3):309-22. doi: 10.1016/j.ccr.2012.02.022. PMID: 224399266. Klemm F, Joyce JA. Microenvironmental regulation of therapeutic response in cancer. Trends Cell Biol. 2015 Apr;25(4):198-213. doi: 10.1016/j.tcb.2014.11.006. Epub 2014 Dec 22. PMID: 25540894; PMCID: PMC5424264.
7. Zhou AK, Jou E, Lu V, et al. Using Pre-Clinical Studies to Explore the Potential Clinical Uses of Exosomes Secreted from Induced Pluripotent Stem Cell-Derived Mesenchymal Stem cells. Tissue Eng Regen Med. 2023 Oct;20(6):793-809. doi: 10.1007/s13770-023-00557-6. Epub 2023 Aug 31. PMID: 37651091; PMCID: PMC10519927.
8. Wu Z, Su Y, Li J, et al. Induced pluripotent stem cell-derived mesenchymal stem cells: whether they can become new stars of cell therapy. Stem Cell Res Ther. 2024 Oct 16;15(1):367. doi: 10.1186/s13287-024-03968-x. PMID: 39415276; PMCID: PMC11484330.
9. ASCO 2025 Annual Meeting. Engineering iPSC-derived mesenchymal stem cells (i MSCs) to secrete IL-7/IL-15 for modulation of the tumor microenvironment in a “cold” ovarian tumor model. https://meetings.asco.org/abstracts-presentations/246879
10. Pittenger MF, Discher DE, Péault BM, et al. Mesenchymal stem cell perspective: cell biology to clinical progress. NPJ Regen Med. 2019 Dec 2;4:22. doi: 10.1038/s41536-019-0083-6. PMID: 31815001; PMCID: PMC6889290.11. National Cancer Institute: Surveillance, Epidemiology, and End Results Program. Cancer Stat Facts: Ovarian Cancer, https://seer.cancer.gov/statfacts/html/ovary.html.










No comments yet