



Organ-on-chip models are gaining attention across pharma as tools for studying disease and predicting drug responses. Professor Donald Ingber of the Wyss Institute at Harvard University discusses how these systems could help improve confidence in early drug discovery.
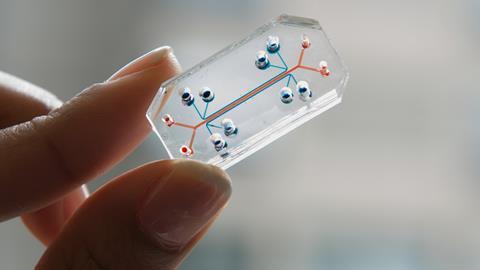
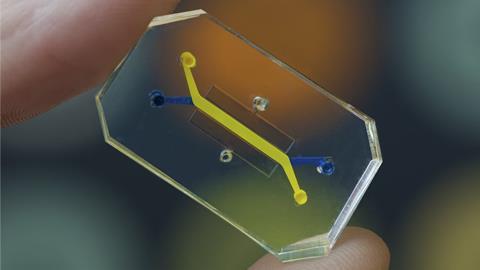
Over the past two decades, organ-on-chip technologies have developed from an experimental concept into a growing platform for modelling human disease and evaluating drug responses. These microfluidic devices are lined with living human cells and recreate key aspects of tissue structure, fluid flow and mechanical forces. By reproducing elements of organ physiology in vitro, they enable researchers to study biological processes that are difficult to capture using conventional cell culture models.
Among the pioneers of this approach is Professor Donald E Ingber, Founding Director of the Wyss Institute at Harvard University and a professor with appointments at Harvard Medical School and the Harvard John A Paulson School of Engineering and Applied Sciences. His laboratory has played a central role in developing organ-on-chip technology and demonstrating its potential for modelling disease, supporting drug discovery research and advancing personalised medicine.
Ingber also helped co-found Emulate Inc., a company developing organ chip platforms for biomedical research and pharmaceutical development. His research now focuses on advancing these systems and exploring how they can be used to model human physiology and disease in ways that support drug discovery.
A window into disease mechanisms
Organ chips are designed to replicate the structure and function of human tissues within a microengineered environment. Living human cells are cultured in microfluidic devices that recreate important physiological features such as tissue interfaces, fluid flow and mechanical forces.
These systems allow researchers to study disease biology in a human-relevant context. As Ingber explained:
“Organ chips provide a powerful way to analyse cellular, molecular and biophysical mechanisms of disease in a human-relevant manner and hence to identify clinically relevant drug targets.”
According to Ingber, the platforms enable researchers to vary multiple contributors to disease, including immune cells, signalling molecules, hormones, oxygen levels and the microbiome. These factors can be examined individually or in combination with cellular responses being monitored in real time. This makes it possible to study biological processes across several levels, from tissue interactions down to molecular signalling pathways.
Ingber described the systems as offering direct visibility into cellular activity within a tissue context:
“They essentially provide a ‘window’ on molecular-scale activities within living human cells while in a physiologically relevant tissue and organ context.”
He revealed that this approach has supported the identification of therapeutic targets, the repurposing of existing drugs and the evaluation of new compounds in human-relevant systems. He added that organ chip studies have also revealed important roles for mechanical forces in disease processes, with implications for both disease modelling and drug target identification.
How organoids and organ chips work together
Organoids have become an established approach for modelling human tissues and Ingber said his group uses them, particularly as a source of cells. He described organoids created from adult-tissue stem cells isolated from patient organs as “an outstanding source of cells” because they can be expanded in 3D gel cultures. He added that these organoid-derived cells can then be dissociated and combined with other tissue types in organ chips to form more complex organ-level structures.
“Organoid cultures currently can be carried out at higher throughput than most organ-chip models and so they can be used as a rapid first screening method for assessing drug efficacy and safety,” he says.
However, he stressed that the chip environment can change how cells behave compared with organoid culture alone. Ingber noted that his team has observed different responses when the same organoid-derived cells are cultured with other tissue types in microfluidic organ-chip systems, which is why he does not view organoids and organ chips as competing approaches.
Organoid cultures currently can be carried out at higher throughput than most organ-chip models and so they can be used as a rapid first screening method for assessing drug efficacy and safety.
He gave the intestine as an example. Ingber explained that intestinal organoids grow as closed balls of cells, which makes several functional readouts difficult to quantify. He listed absorption, transport, secretion and mucus accumulation as examples and added that extended co-culture with the human microbiome is also difficult in those closed structures. These types of analyses, he said, can be carried out on a chip and his group has already used organ-chip systems to perform them.
Another difference he highlighted is control over drug exposure. Ingber said organ chips experience dynamic fluid flow, which allows researchers to reproduce clinically relevant pharmacokinetic profiles, meaning drug levels that rise and fall over time in the bloodstream. This matters, he argued, because a single static dose applied in a culture dish does not reflect how tissues encounter drugs in patients.
Increasing confidence by testing against clinical results
When asked how organ chips can support better early discovery decisions, Ingber framed the issue in terms of validation against human clinical outcomes. Rather than treating basic functionality as sufficient, he said his group compares results generated in organ chips directly with findings from clinical studies in patients. This approach, which he described as “clinical mimicry”, is used as a benchmark for evaluating model performance.
Ingber said the same principle applies to toxicity studies. The aim, he explained, is not simply to demonstrate that a tissue model can be maintained in culture, but to determine whether it can reproduce adverse responses observed in humans.
As an example, he pointed to a human Liver Chip study that examined the responses of 27 drugs with known safety profiles in animals and humans, including compounds where the two systems produce different results. According to Ingber, the organ-chip model accurately predicted drug-induced liver injury observed in patients and outperformed conventional animal models.
“This predictive power was more than seven times more accurate than the animal models had been,” he explained.
Results such as these support the use of organ-chip systems earlier in drug discovery programmes, when decisions about candidate selection and series progression can have significant downstream consequences.
Why interfaces, flow and forces matter
Organ-chip systems are designed to incorporate physiological features that are missing from most preclinical culture models. Ingber argued that several of these elements have direct consequences for drug responses.
One example is the presence of tissue interfaces. Ingber cited epithelial–stromal interactions as a long-recognised driver of tissue and organ development. Ingber noted that these interfaces are absent from many conventional culture models, which can limit tissue differentiation and alter disease behaviour. In inflammatory bowel disease (IBD), he explained, the stroma can be a major driver of inflammation and may increase the tendency for cancer formation in the epithelium. Ingber added that stromal fibroblasts have emerged as major drivers of inflammation in IBD in his group’s studies, while many existing drugs focus on the epithelium or immune cells.
He also emphasised the importance of fluid flow. According to Ingber, flow supports tissue differentiation and long-term viability in organ-chip systems. As an example, he noted that primary human hepatocytes lose specialised functions within one to three days in conventional culture, whereas his team retains in vivo-like functionality for one to two weeks when flow is maintained on a chip.
Mechanical forces were another factor Ingber frequently returned to. As he explained:
“We also have repeatedly found that mechanical forces – for example, those associated with breathing in lung and peristalsis in intestine – play fundamental roles in healthy physiology and in the development of various disease states.”
These forces can influence disease processes in several ways. Ingber pointed to examples from organ-chip studies showing that physical motion can alter inflammatory responses, infection dynamics and tissue behaviour.
We also have repeatedly found that mechanical forces – for example, those associated with breathing in lung and peristalsis in intestine – play fundamental roles in healthy physiology and in the development of various disease states.
“Breathing motions increase inflammation induced by smog-like nanoparticles but suppress viral infection and tumour growth.”
Peristaltic movements, he said, can suppress overgrowth by gut microbes and enhance mucus production. At the same time, Ingber noted that peristalsis can exacerbate fibrosis and inflammation in intestine chips lined with tissue from women with IBD when pregnancy hormones are present, mirroring symptom exacerbation reported in some pregnant patients.
Observations such as these can reveal previously unrecognised therapeutic targets. He cited pulmonary oedema and virus-induced inflammation in the lung as examples where his group has shown that organ-chip studies can lead to the identification of new targets. Findings like these, he suggested, can also prompt researchers to re-examine assumptions about the biological drivers of disease.
Regulatory developments
Organ chips are being explored widely across the pharmaceutical sector but have not yet been integrated into routine drug development pipelines. Many pharmaceutical and biotechnology companies are currently evaluating new approach methodologies (NAMs) within their internal research laboratories, including organ-chip systems.
Regulatory developments may also accelerate this transition. Ingber pointed to a recent roadmap announced by the US Food and Drug Administration (FDA) aimed at encouraging a move away from animal studies towards alternative experimental approaches.
“Virtually all the major pharma/biotech companies and many of the smaller ones are actively exploring the use of new approach methodologies, including organ chips in their internal labs.”
According to Ingber, the roadmap highlights Emulate’s Liver Chip study as an example of the type of work needed to support regulatory adoption. He explained that the study is being used to move the platform through the FDA’s Innovative Science and Technology Approaches for New Drugs (ISTAND) qualification programme, which evaluates new technologies that could eventually replace certain animal experiments.
What needs to change next
On what needs to improve for organ chips to have a larger role in drug discovery, Ingber focused on practical implementation. He said the most important advances include “Higher throughput, lower cost, automated organ-chip culture systems integrated with in-line imaging, sensors, AI and computational modelling.”
He presented this as an engineering and workflow problem as much as a biological one. Higher throughput and automation matter for adoption, he argued, because routine use requires reproducibility, scalability and integration with existing screening and analytics.
A tool for targeted questions, not a replacement for everything
Organ chips are most useful when the biological question depends on human-tissue context, multicellular interactions, exposure dynamics and physical forces that conventional models do not capture well. They make it possible to vary disease contributors systematically and measure responses from tissue level down to molecular readouts in real time. Studies using these systems have supported target identification, drug repurposing and compound evaluation where comparisons with clinical data are possible. They also have enabled clinicians to predict individual patient responses to cancer therapies when the drugs were perfused through the chips using a clinically relevant administration regimen.
Adoption is increasing, but routine integration into drug development pipelines will depend on improvements in throughput, cost and automation, alongside continued validation against human clinical data.













No comments yet